Overview
 An Achilles tendon rupture is also known as a rupture of the gastrocnemius tendon, or the common calcanean tendon. The tendon is actually composed of 5 different tendons, the two most important being the superficial digital flexor and gastrocnemius tendons. The gastrocnemius tendon is the largest of these, and is the most powerful extensor of the hock (ankle) joint. Both the superficial digital flexor and gastrocnemius tendons attach to the heel bone, called the calcaneus bone. A rupture of the Achilles tendon may be a partial tear, which means just the gastrocnemius is torn, or a complete tear, in which all five tendons have been torn. (show diagrams, normal anatomy vs partial vs complete tears).
An Achilles tendon rupture is also known as a rupture of the gastrocnemius tendon, or the common calcanean tendon. The tendon is actually composed of 5 different tendons, the two most important being the superficial digital flexor and gastrocnemius tendons. The gastrocnemius tendon is the largest of these, and is the most powerful extensor of the hock (ankle) joint. Both the superficial digital flexor and gastrocnemius tendons attach to the heel bone, called the calcaneus bone. A rupture of the Achilles tendon may be a partial tear, which means just the gastrocnemius is torn, or a complete tear, in which all five tendons have been torn. (show diagrams, normal anatomy vs partial vs complete tears).
Causes
The exact cause of Achilles tendon ruptures is hard to say. It can happen suddenly, without warning, or following an Achilles tendonitis . It seems that weak calf muscles may contribute to problems. If the muscles are weak and become fatigued, they may tighten and shorten. Overuse can also be a problem by leading to muscle fatigue . The more fatigued the calf muscles are, the shorter and tighter they will become. This tightness can increase the stress on the Achilles tendon and result in a rupture. Additionally, an imbalance of strength of the anterior lower leg muscles and the posterior lower leg muscles may also put an athlete at risk for an injury to the Achilles tendon. An Achilles tendon rupture is more likely when the force on the tendon is greater than the strength of the tendon. If the foot is dorsiflexed while the lower leg moves forward and the calf muscles contract, a rupture may occur. Most ruptures happen during a forceful stretch of the tendon while the calf muscles contract. Other factors that may increase the risk of Achilles tendon rupture include. Tight calf muscles and/or Achilles tendon. Change in running surface eg: from grass to concrete. Incorrect or poor footwear. A change of footwear eg: from heeled to flat shoes. It is thought that some medical conditions, such as gout, tuberculosis and systemic lupus erythematosus, may increase the risk of Achilles tendon rupture.
Symptoms
Symptoms include a sudden sharp pain in the achilles tendon which is often described as if being physically struck by an object or implement. A loud snapping noise or bang may also be heard at the time. A gap of 4 to 5 cm in the tendon can be felt which may be less obvious later as swelling increases. After a short while the athlete may be able to walk again but without the power to push off with the foot. There will be a significant loss of strength in the injured leg and the patient will be unable to stand on tip toes. There may be considerable swelling around the achilles tendon and a positive result for Thompson's test can help confirm the diagnosis.
Diagnosis
The doctor may look at your walking and observe whether you can stand on tiptoe. She/he may test the tendon using a method called Thompson?s test (also known as the calf squeeze test). In this test, you will be asked to lie face down on the examination bench and to bend your knee. The doctor will gently squeeze the calf muscles at the back of your leg, and observe how the ankle moves. If the Achilles tendon is OK, the calf squeeze will make the foot point briefly away from the leg (a movement called plantar flexion). This is quite an accurate test for Achilles tendon rupture. If the diagnosis is uncertain, an ultrasound or MRI scan may help. An Achilles tendon rupture is sometimes difficult to diagnose and can be missed on first assessment. It is important for both doctors and patients to be aware of this and to look carefully for an Achilles tendon rupture if it is suspected.
Non Surgical Treatment
Non-surgical treatment typically involves wearing a brace or cast for the first six weeks following the injury to allow time for the ends of the torn tendon to reattach on their own. Over-the-counter medications, such as ibuprofen or aspirin, may be taken during this time to reduce pain and swelling. Once the tendon has reattached, physical therapy will be needed to strengthen the muscles and tendon. A full recovery is usually made within four to six months.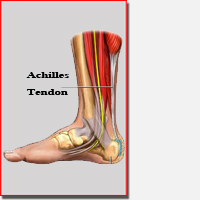
Surgical Treatment
Surgery to repair an Achilles tendon rupture is performed under a spinal or general anaesthetic. During surgery the surgeon makes an incision in the skin over the ruptured portion of the tendon. The tendon ends are located and joined together with strong sutures (stitches), allowing the tendon to closely approximate its previous length. The skin is then closed with sutures and the foot is immobilised in a cast or splint, again in the toes-pointed position. Seven to ten days after surgery the cast or splint is removed in order for the sutures in the skin to be removed. Another cast or splint will be applied and will stay in place a further 5 - 7 weeks.
An Achilles tendon rupture is also known as a rupture of the gastrocnemius tendon, or the common calcanean tendon. The tendon is actually composed of 5 different tendons, the two most important being the superficial digital flexor and gastrocnemius tendons. The gastrocnemius tendon is the largest of these, and is the most powerful extensor of the hock (ankle) joint. Both the superficial digital flexor and gastrocnemius tendons attach to the heel bone, called the calcaneus bone. A rupture of the Achilles tendon may be a partial tear, which means just the gastrocnemius is torn, or a complete tear, in which all five tendons have been torn. (show diagrams, normal anatomy vs partial vs complete tears).Causes
The exact cause of Achilles tendon ruptures is hard to say. It can happen suddenly, without warning, or following an Achilles tendonitis . It seems that weak calf muscles may contribute to problems. If the muscles are weak and become fatigued, they may tighten and shorten. Overuse can also be a problem by leading to muscle fatigue . The more fatigued the calf muscles are, the shorter and tighter they will become. This tightness can increase the stress on the Achilles tendon and result in a rupture. Additionally, an imbalance of strength of the anterior lower leg muscles and the posterior lower leg muscles may also put an athlete at risk for an injury to the Achilles tendon. An Achilles tendon rupture is more likely when the force on the tendon is greater than the strength of the tendon. If the foot is dorsiflexed while the lower leg moves forward and the calf muscles contract, a rupture may occur. Most ruptures happen during a forceful stretch of the tendon while the calf muscles contract. Other factors that may increase the risk of Achilles tendon rupture include. Tight calf muscles and/or Achilles tendon. Change in running surface eg: from grass to concrete. Incorrect or poor footwear. A change of footwear eg: from heeled to flat shoes. It is thought that some medical conditions, such as gout, tuberculosis and systemic lupus erythematosus, may increase the risk of Achilles tendon rupture.
Symptoms
Symptoms include a sudden sharp pain in the achilles tendon which is often described as if being physically struck by an object or implement. A loud snapping noise or bang may also be heard at the time. A gap of 4 to 5 cm in the tendon can be felt which may be less obvious later as swelling increases. After a short while the athlete may be able to walk again but without the power to push off with the foot. There will be a significant loss of strength in the injured leg and the patient will be unable to stand on tip toes. There may be considerable swelling around the achilles tendon and a positive result for Thompson's test can help confirm the diagnosis.
Diagnosis
The doctor may look at your walking and observe whether you can stand on tiptoe. She/he may test the tendon using a method called Thompson?s test (also known as the calf squeeze test). In this test, you will be asked to lie face down on the examination bench and to bend your knee. The doctor will gently squeeze the calf muscles at the back of your leg, and observe how the ankle moves. If the Achilles tendon is OK, the calf squeeze will make the foot point briefly away from the leg (a movement called plantar flexion). This is quite an accurate test for Achilles tendon rupture. If the diagnosis is uncertain, an ultrasound or MRI scan may help. An Achilles tendon rupture is sometimes difficult to diagnose and can be missed on first assessment. It is important for both doctors and patients to be aware of this and to look carefully for an Achilles tendon rupture if it is suspected.
Non Surgical Treatment
Non-surgical treatment typically involves wearing a brace or cast for the first six weeks following the injury to allow time for the ends of the torn tendon to reattach on their own. Over-the-counter medications, such as ibuprofen or aspirin, may be taken during this time to reduce pain and swelling. Once the tendon has reattached, physical therapy will be needed to strengthen the muscles and tendon. A full recovery is usually made within four to six months.
Surgical Treatment
Surgery to repair an Achilles tendon rupture is performed under a spinal or general anaesthetic. During surgery the surgeon makes an incision in the skin over the ruptured portion of the tendon. The tendon ends are located and joined together with strong sutures (stitches), allowing the tendon to closely approximate its previous length. The skin is then closed with sutures and the foot is immobilised in a cast or splint, again in the toes-pointed position. Seven to ten days after surgery the cast or splint is removed in order for the sutures in the skin to be removed. Another cast or splint will be applied and will stay in place a further 5 - 7 weeks.
